
JOHN LI, M.D.
OTOLOGY NEUROTOLOGY RESOURCES
210 Jupiter Lakes Blvd #5105
Jupiter, FL 33458
Phone: (561)-748-4445
Fax: (561)-748-4449
Surgical Treatment OF Meniere's Syndrome or Endolymphatic Hydrops
Review Definition: Meniere’s syndrome and endolymphatic hydrops both refer to a condition of excess pressure accumulation in the endolymph which causes the following symptoms:
| Fluctuating hearing loss (hearing that is good sometimes and bad sometimes) | |
| Occasional vertigo (usually a spinning sensation, sometimes violent) | |
| Tinnitus or ringing in the ears (usually low tone roaring / ocean-like) |
| Aural fullness (pressure sensation in the ears) |
Physiology: There are two fluids that fill the chambers of the inner ear. These fluids are called endolymph and perilymph, and are separated by thin membranes that contain nerve tissue. Fluctuations in the pressure of these fluids will stretch these nerve-filled membranes and may cause hearing disturbance, ringing in the ears, vertigo, imbalance and a pressure sensation in the ear. Read more on Meniere's at this E-Medicine Article.
Note that Surgery is reserved for failure of more conservative therapies such as Dietary management, Medical management and Oral Steroid management.
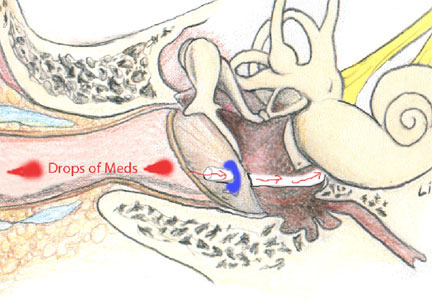
Steroid Perfusion: An outpatient tube insertion procedure. Steroid medication is applied through the tube (minor surgery) into the inner ear. This gets a higher concentration of medication to the ear and avoids systemic side effects. It is relatively noninvasive and can be used to recover hearing.
Meniett: This is a new treatment where an air pressure generator is applied to the ear on a daily basis. It requires insertion of a tympanostomy tube. It is noninvasive but high cost (device equals $3600). (Control, not cure.)
Endolymphatic Sac Decompression / Shunt:
Decreases the pressure build up of the endolymph by removing bone that encases the endolymph reservoir. This allows the reservoir sac to expand more freely and allows the pressure to dissipate. This has approximately a 60-80 % chance of (1) controlling vertigo (2) stabilizing and preserving hearing acuity. The surgery involves a mastoidectomy approach. The recovery period is usually short and uneventful, with minimal pain.
Aminoglycoside Perfusion: An outpatient procedure. An antibiotic that is toxic specifically to the balance nerve is placed through a small puncture in the eardrum. This antibiotic essentially kills the balance nerve and usually (95%) spares the hearing. Success has been reported to be about 90% although relapses are possible.
Vestibular Nerve Section: For patients with useful hearing in both ears, cutting the diseased balance nerve can often cure the symptoms. This has the advantage of a high cure rate (about 97 %) and can preserve hearing in the operated ear. The surgery involves both an otologist and a neurosurgeon and is more complex than the endolymphatic sac decompression.
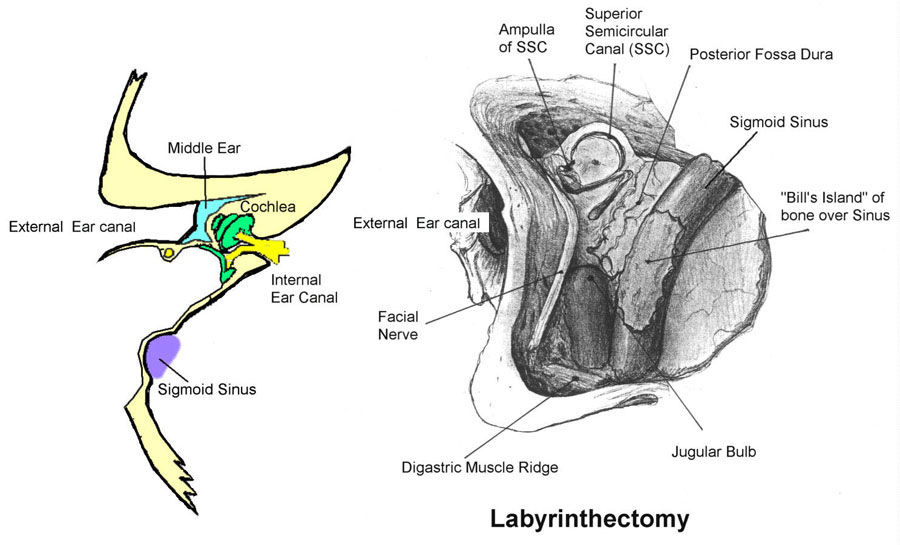
Labyrinthectomy: Has the advantage of a high cure rate, (greater than 97 %) and is useful in the patient whose hearing on the diseased side has already been destroyed by Meniere's disease. It involves removal of the diseased inner ear organs but does not require entry into the cranial cavity and is thus less complex than the vestibular nerve section.